Disease Awareness: Colorectal Cancer
March is Colorectal Cancer Awareness Month!
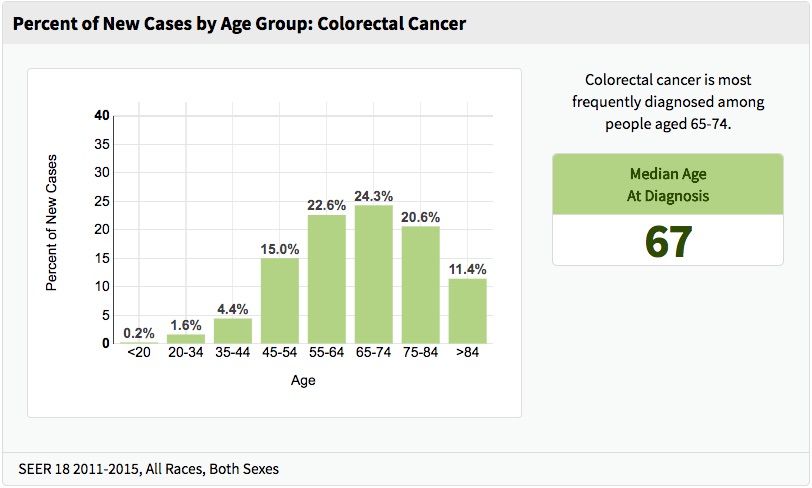
March is Colorectal Cancer Awareness month! It's important for people to know that detection is vital to prevention and early diagnosis—the CDC recommends anyone 50 years or older be screened for precancerous polyps. If you or a relative has had CRC, if you have Crohn’s disease or ulcerative colitis, or have certain genetic syndromes such as familial adenomatous polyposis (FAP) or Lynch Syndrome, you may need to be tested earlier than 50 years old, and/or more frequently than the general population, as your chances for developing CRC are higher. As with most cancers, the risk of colorectal cancer increases with age. In fact, 90% of colorectal cases occur in people 50 years or older.
Similar to other cancers, the lifestyle factors that can contribute to your risk of CRC include: alcohol consumption, tobacco use, obesity, high processed fat/low fruit and vegetable diets, and lacking physical exercise. The good news is, these factors can help reduce your risk for CRC: follow a diet rich in fruits and vegetables, get adequate exercise (the American Heart Association, among others, recommends 150 minutes of exercise per week for adults), and limit alcohol and tobacco use. There is also evidence that a low-dose aspirin regimen decreases CRC risk. Above all, regular screening will help detect CRC and remove polyps before they become cancerous. Common symptoms for colorectal cancer include nausea and vomiting, loss of appetite, constipation, and blood in the stool for those over 50. However, 50% of those with CRC do not report any symptoms. Again, CRC screening is key!
Doctors are as optimistic as ever about treating CRC. The rise of immunotherapy has been instrumental in improving progression free and overall survival in many cancers and CRC was one of the first cancers in which PDL-1/PD1 inhibitors were approved. Many questions on theMednet are focused on immunotherapy for metastatic disease or the duration of adjuvant chemotherapy for locally advanced disease. Check out some of the recent CRC questions on theMednet, and keep coming back for new Q&A on CRC treatment options!